















 49 / 68
49 / 68

Vol 5 No 5 October/November 2016
Australian Journal of Dementia Care
49
will depend on the behaviours which are
the target of the program, using theory
may guide the program’s steps.
Consider staff motivation as well as
knowledge and skills – why would staff
want to change, what’s in it for them?
We are still building our understanding
about the drivers of practice change, and
how to study and report outcomes. From
our review we recommend that studies
need to pay attention to ‘program logic’ –
the picture of why and how a strategy is
proposed to work and assumptions about
cause and effect (see our paper,
referenced at the end of this article, for
specific examples).
Aprogram logic approach ensures an
intervention targets the best areas for staff
and resident change outcomes – for
example, to reduce hip fractures, should
we address both falls risk as well as
protection against fracture if the resident
does fall? Program logic will also help
other teams work out how to implement
a strategy in their own setting.
Changing practice is an important
investment of resources and our review
was an encouraging exploration of the
variety and intensity of effort in dementia
care.
Acknowledgments
This work was supported by the Dementia
Collaborative Research Centres at UNSW
Australia, Queensland University of Technology,
and Australian National University and partly
funded by the DCRC Knowledge Translation
Program.
References
Low L-F, Fletcher J, Goodenough B, Jeon Y-H,
Etherton-Beer C, MacAndrew M, Beattie E
(2015) A systematic review of interventions to
change staff care practices in order to improve
resident outcomes in long-term residential aged
care.
Plos One
epub Nov 11 2015. Available at:
http://journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0140711
Lee-Fay Low is a DCRC: Assessment and
Better Care (ABC) research collaborator and
Associate Professor in Ageing and Health,
University of Sydney; Dr Jennifer Fletcher is a
researcher at the Ageing, Work and Health
Research Unit at Sydney University; Associate
Professor Belinda Goodenough is Senior Visiting
Fellow, DCRCs, UNSW Australia; Professor Yun-
Hee Jeon is a DCRC: ABC research collaborator
and Professor of Chronic Disease and Ageing,
University of Sydney; Christopher Etherton-Beer
is Associate Professor in Geriatric Medicine at the
University of WA; Margaret MacAndrew is a PhD
student with the DCRC: Carers and Consumers
(DCRC: CC); and Professor Elizabeth Beattie is
Director of the DCRC: CC. For more information
contact:
lee-fay.low@sydney.edu.auSee right for an analysis of the Appreciative
Inquiry approach in changing dementia
care practice and service delivery.
“We support progress – it’s the change we don’t
like” (anonymous)
D
o you struggle with breaking a habit?
Feel stuck in a thought pattern? Can’t
make a new routine ‘stick’? People
can find change hard – even when the case
for change is based on proven facts.
Organisations can also find change
difficult. Whether it be implementing new
processes, procedures, positions, or
policies, many change initiatives do not
deliver adequately on their change
objectives and goals. This so-called ‘failure
rate’ has been estimated to be as high as
70%, with research suggesting it is due
partly to the ways that organisations
address people management issues and
individual differences (Probst & Raisch
2005; Caldwell & Liu 2011).
An essential factor in effective change
management is the ability of managers and
change agents to create an appropriate
mindset of ‘change readiness’.
We can think of this mindset as the
degree to which people involved in or
affected by a change are individually and
collectively primed, motivated, and
capable of executing the change (Holt
et al
2010).
Team leaders andmanagers know that
even the smallest changes in dementia care
delivery can be challenging to implement.
Yet, because research-derived knowledge is
continually being tested and updated,
change is a constant expectation of good
practice.
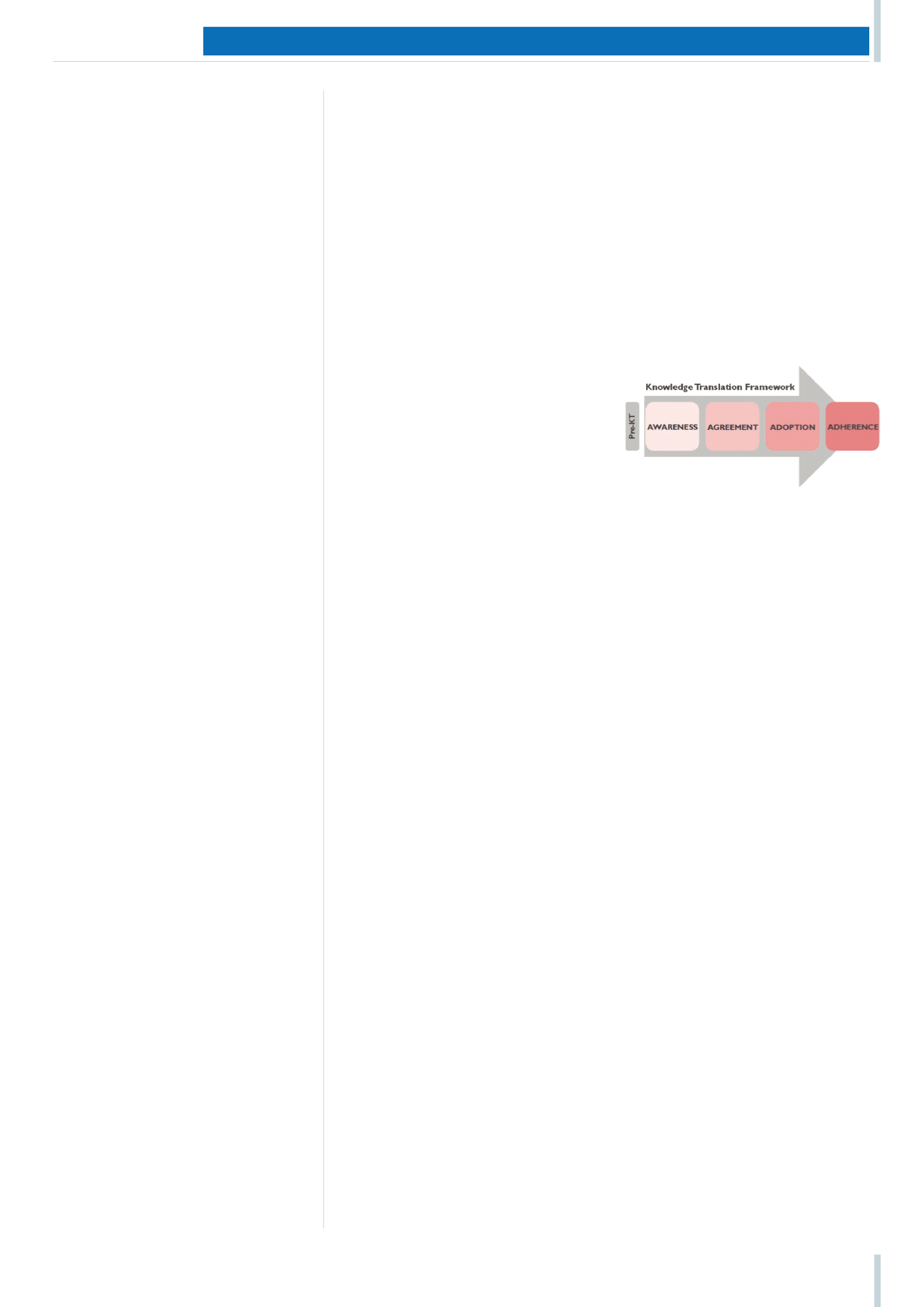
According to the Dementia Training
Study Centres' (DTSCs') Knowledge
Translation (KT) framework, the practice
change journey involves at least four steps
for new knowledge to make a difference to
care (see Figure 1): people need to become
aware
of newmethods, to
agree
this
knowledge is relevant, to
adopt
these new
methods, and then find ways to
adhere
to
(sustain) implementation. This sequence
can take a long time, and also not be as
linear as it sounds!
The DCRCs' KT programworked with
the DTSCs to identify the best ways to
support the KT journey, and the methods
for creating and leading a ‘change’
mindset. One approach gaining popularity
inAustralian organisations is ‘Appreciative
Inquiry’. This article checks the evidence
for the application of this method in
dementia care.
What is Appreciative Inquiry?
With roots in positive psychology and
business management, Appreciative
Inquiry (AI) is a strengths-based
philosophy of change management. AI
aims to guide practice change efforts
around what is working, rather than trying
to fix what isn’t (the problem solving
approach, see box p51).
Abasic tenet of AI is that organisational
culture (‘the way we do things around
here’) reflects the direction that employees
orient their attention. An
appreciative
approach is a deliberate choice to focus
inquiry
(attention) on success, rather than
organisational failures.
This inquiry method is collaborative. It
involves people sharing their views to
reach a common understanding about the
best of ‘what is’, and develop a vision for
future featuring more of that best. TheAI
process has been described as a continuous
cycles of the ‘4Ds’: discovery, dreaming,
designing and destiny (Cooperrider &
Whitney 1999).
Why is it popular?
AI has a positive lens. It can feel good! AI
methods encourage interactive teamwork,
are achievement oriented, with
DCRC SPEC I AL I SSUE : THE B I G P I CTURE I N DEMENT I A RESEARCH
Checking the evidence
for Appreciative Inquiry
Even the smallest changes in dementia care delivery can be
challenging to implement. Appreciative Inquiry is one practice-
change approach that’s gaining popularity in Australian
organisations.
Belinda Goodenough
,
Ruby Tsang
and
Michael Young
investigate how it’s been used in dementia care
settings and with what outcomes
Figure 1: The four-stage knowledge
translation journey of the DTSCs