















 52 / 68
52 / 68

52
Australian Journal of Dementia Care
October/November 2016 Vol 5 No 5
Connections in care count
M
aintaining positive social
connections and feeling socially
supported are associated with
better mental and physical health and
well-being for older adults living in the
community (Ashida & Heaney 2008;
NSPAC 2013).
Many older adults who move into
long-term care (ie residential aged care,
nursing homes, care homes) report that
changes in their social relationship
networks are among the most
challenging aspects of their relocation
(Bradshaw
et al
2012). Over 52% of
people living in long-term care in
Australia have a dementia diagnosis
noted (AIHW 2015). Adapting to new
social relationships in care is particularly
challenging for people with dementia
who may have impaired memory and
reduced functional capacity (Doyle
et al
2011).
In Australia, people with dementia live
in residential care for an average of 3.25
years (AIHW 2015). Residents necessarily
form new networks of diverse
relationships including those with other
residents, care staff, visiting therapists,
and even other residents’ family
members (Kovach & Robinson 1996;
Wilson
et al
2009). While current
principles and policies in care favour a
holistic approach that addresses the
physical, psychological and social needs
of people with dementia (AHMAC 2005),
their social connections in care are rarely
considered or documented (Reed &
Payton 1997; Theurer
et al
2015).
We are two PhD candidates from the
Dementia Collaborative Research Centre:
Assessment and Better Care, UNSW
Australia, who are conducting separate
studies using social network analysis to
investigate ways in which the networks
of people with dementia in long-term
care are associated with their care, well-
being and perceptions of support or
isolation.
The first study, the SOCIAL (Social
Orientation of Care in Aged Living) (led
by Janet), is researching the social-
professional networks of selected
residents with dementia in four long-
term care settings in the Sydney region.
The study, which is running until
December 2017, aims to identify possible
associations between each resident’s in-
house connections and their care,
neuropsychiatric symptoms, and use of
psychotropic medications (Mitchell
et al
2015).
The second study, the Friendship and
Relationship Interactions in the Elderly
Networks Description (FRIEND, led by
Anne-Nicole), which finished earlier this
year, explored the structure, meaning
and influence of social relationships
between residents living in three high-
care units of a Sydney long-term care
home, including a dementia specific unit
(Casey
et al
2015). This article provides a
brief explanation of social network
analysis, an overview of results from the
studies to date, and implications for the
care of people with dementia.
Why social network analysis?
Social network analysis (SNA) is an
innovative method for exploring the
structure and qualities of different types
of long-term care-based relationships
experienced by residents with dementia,
and for describing the social
environment in which they live. Whereas
traditional data describe people in terms
of their individual attributes, SNAdata
describe people in terms of their social
roles and relationships (Hanneman &
Riddle 2005).
Identifying how people connect
together (network structure) and the
quality of their relationships – whether
positive or negative, mutual or one-
sided, strong bonds or just ‘people we
know’ – can help care staff and care
providers understand how these
relationships benefit or constrain the
people involved (Abbott
et al
2015). SNA
data address questions about the size of
networks, the social distance (‘degrees of
separation’) between people, and how
things as diverse as knowledge, illness,
and emotions flow through social
networks (Cornwell & Waite 2009; van
Beek
et al
2011).
Social-professional networks in care
The SOCIAL study conducted a
systematic literature review of studies
that have used SNA and involved people
with dementia in long-term care. Results
indicate residents have small close
personal networks (Mitchell
et al
2015).
One of the studies included in that
literature review analysed the size of
networks of people in 13 care homes in
rural NSW, where over half the residents
DCRC SPEC I AL I SSUE : THE B I G P I CTURE I N DEMENT I A RESEARCH
Anne-Nicole Casey
and
Janet Mitchell
are using social network analysis (SNA) in their research to
investigate and describe the relationship networks of people with dementia living in long-term residential
care. Their results are truly concerning, revealing profound social isolation among residents and
highlighting the need for staff to create oases of supportive connections
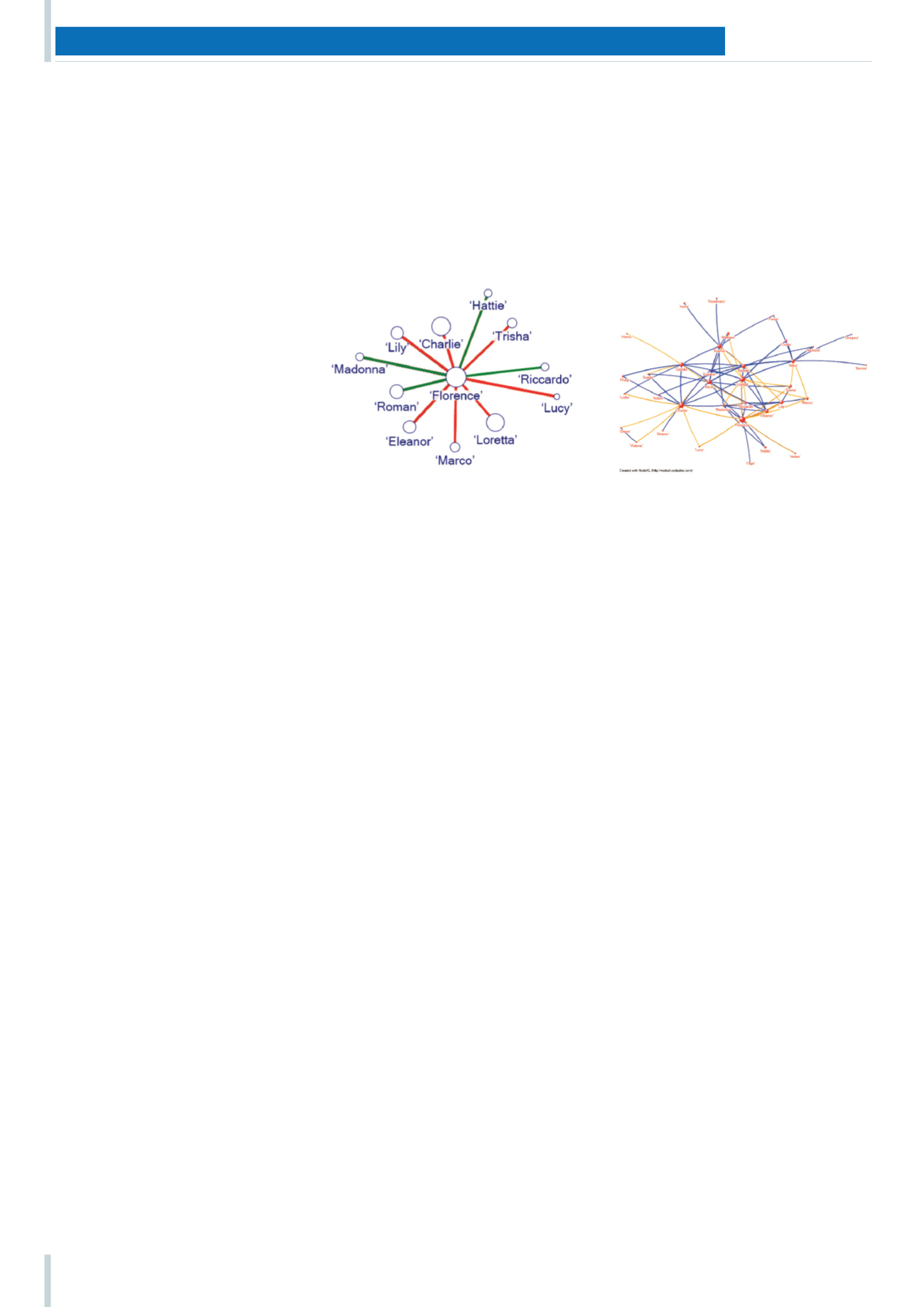
Using SNA data to illustrate social networks: In these examples of graphed network data
from the FRIEND study, circles represent people and lines represent relationships between
people living in a Sydney long-term care home. Figure A (left) illustrates ‘egocentric’ data.
This type of graph represents one person (‘Florence’) and her relationships with people from
different groups. In this example larger circles represent frequent interaction partners,
green lines represent supportive relationships, and red lines represent antagonistic
relationships. Figure B illustrates ‘sociocentric’ data from a larger ‘bounded’ network. This
type of graph illustrates relationships between people within a defined group, such as
people living together in a residential care unit.
Figure A
Figure B