















 61 / 68
61 / 68

Vol 5 No 5 October/November 2016
Australian Journal of Dementia Care
61
Difficulties with suggesting
or implementing change
Organisational management,
structure and culture
Consistent with the work of
others (Cooke
et al
2014;
Phillipson
et al
2016),
participants reported that a
lack of support from
management
and/or senior
staff was a key barrier to their
ability to suggest and trial
changes. Management were
often viewed as not interested
in, or not in agreement with,
suggestions from direct care
staff. A lack of effective
consultation, follow up and
feedback where suggestions
were made was also reported.
One participant noted: “… I
wrote a letter recommending
changes in a secure unit and I
knew there was funding
available. There was no reply
frommanagement and nothing
happened.”
In some cases an
organisational culture
which
lacked flexibility in practice and
approach to dementia care,
existing
policies and
procedures
and the
hierarchical
structure
within organisations
were seen as discouraging of
suggestions regarding different
ways of approaching BPSD
management.
The shifting nature of the
dementia care workforce
was
raised as being inconsistent
with implementing changes
systematically. Specifically,
variable shift structure, high
staff turnover, rigid care
routines, staff fatigue/burnout
and frequent rotation of staff
from one area of the workplace
to another (daily in some cases)
reportedly limit motivation to
suggest and implement
changes. As a result care staff
may not be invested in
changing practice.
Direct care staff factors
Staff attitude
was often seen as
resistant toward change.
Change in practice was
sometimes perceived as too
difficult to implement or not
worth the effort. Fear of change
and wanting to “stay in their
comfort zone” was reported.
Staff members who had been
working in an organisation for
an extended period were
thought to be “set in their
ways”. The potential for “long-
term staff to instil ‘old ways’ in
new staff” was seen as
problematic in that resistance to
trialling new approaches to
BPSDmanagement persisted.
Participants also indicated that
bullying of newer staff
sometimes occurred where they
were set up to fail when
attending to the most “difficult”
residents.
Difficulties around
communication
within the
workplace and relevant
information not being passed
on were repeatedly raised as
barriers. Specifically,
communication breakdown was
linked to:
• not reading resident/client
notes and/or care plans
• information not recorded
• insufficient information
provided at staff handover
• communication limitations
due to language and cultural
differences between staff
members as well as between
staff and people with
dementia
Participants noted issues with
identifying BPSD
management strategies
as such,
and thus not passing the
information on to others (eg
providing a light breakfast at
6am calmed a resident who
would otherwise call out
DCRC SPEC I AL I SSUE : THE B I G P I CTURE I N DEMENT I A RESEARCH
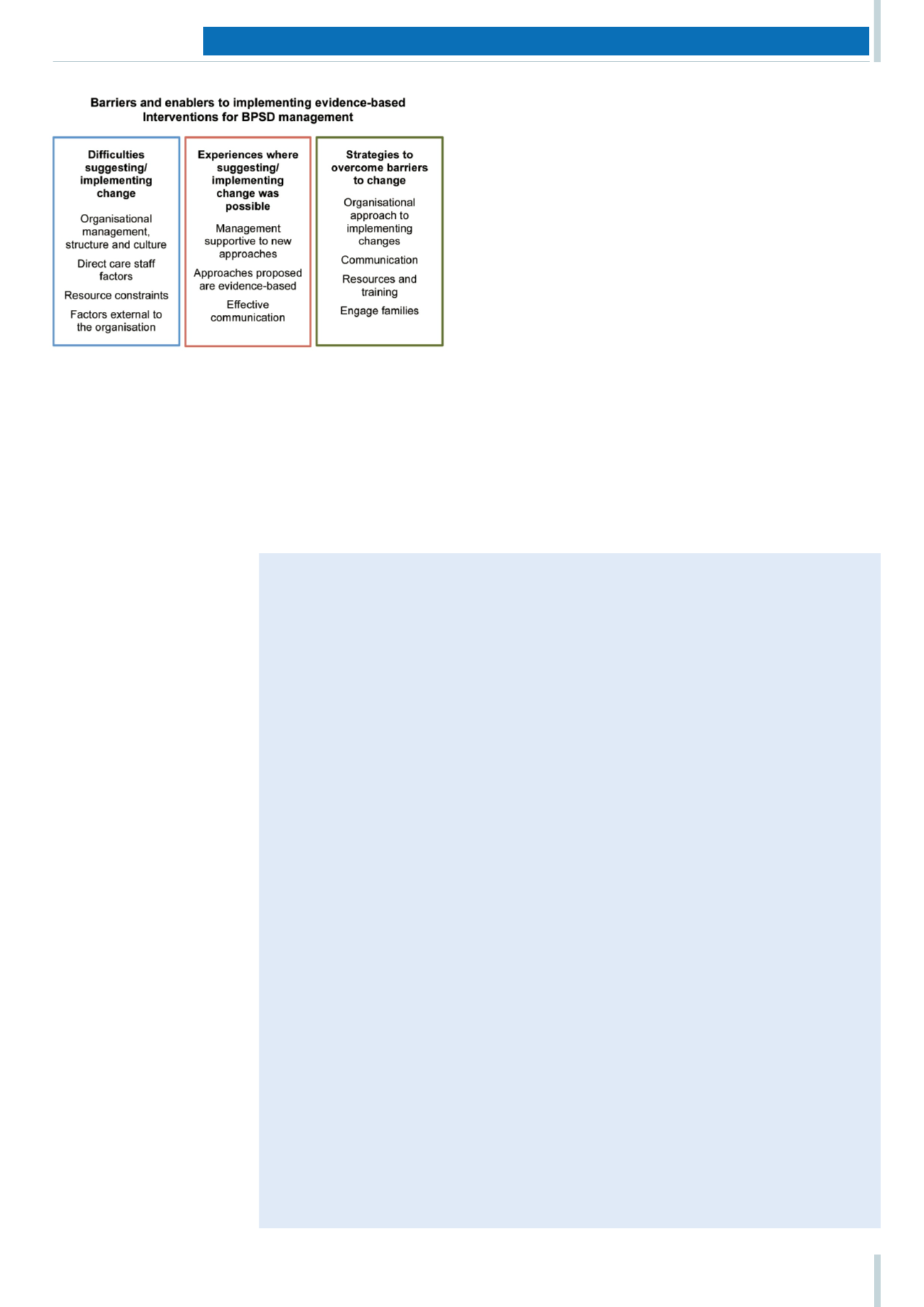
Figure 1: A summary of participant feedback on the barriers and enablers
to implementing evidence-based interventions for BPSDmanagement
Barriers and enablers to KT in health care
In our review of the academic literature* we identified the following barriers and enablers to knowledge
translation (KT) in health care.
Barriers
The four main categories of barriers to successful KT in health care are:
• accessibility of research findings
• anticipated outcomes of using research
• organisational support to use research
• support from others to use research (Retsas 2000).
A lack of authority and limited time to implement change as well as a lack of organisational support are
often reported by health professionals as the greatest barriers to KT (Phillipson
et al
2016; Retsas 2000;
Carlson
et al
2008; Malik
et al
2015; Chau
et al
2008; Atkinson
et al
2008).
Evidence-based practice is not always seen as a core component of clinical care (Harding
et al
2014).
A lack of awareness of the current research and a lack of confidence to evaluate the quality of research
outcomes are also ranked high on the list of barriers (Retsas 2000; Atkinson
et al
2008; McKenna
et al
2005; Draper
et al
2009; Grant
et al
2012).
The
BPSD Guide
provides access to synthesised evidence with all research outcomes rated for quality
of the evidence.
Enablers
The literature also outlines enablers for evidence-based practice. These include:
• Providing integrated, multimodal education that meets the goals of the organisation (Nayton
et al
2014; Chesney
et al
2011).
• Initiating discussion among colleagues to reach consensus around changes to practice (Berland
et
al
2012).
• Providing ready access to research outcomes (Atkinson
et al
2008) and KT strategies tailored to
specific barriers in a specific participant group and setting (Grimshaw
et al
2012; Nayton
et al
2014;
Baker
et al
2010).
• KT strategies are more likely to be successful where the approach is informed by an understanding
of the probable barriers and enablers specific to the context (Grimshaw
et al
2012; Rosen
et al
2002;
Low
et al
2015; Baker
et al
2015; Grol & Grimshaw 2003).
* Details of the literature review are available on request by emailing Kim Burns at
k.burns@unsw.edu.au.