















 17 / 68
17 / 68

Vol 5 No 5 October/November 2016
Australian Journal of Dementia Care
17
Achieving our vision
Amultifaceted, whole organisation
approach has been required to achieve
our vision. Our program integrates four
key elements: clinical leadership; lifestyle
programs and tailored support for
residents; ongoing family assistance; and
supportive physical environments.
Clinical leadership
We’ve appointed senior Registered
Nurses as Clinical Leaders (residents’
case managers) at every facility to
coordinate care and drive our program
philosophy. Registered and Enrolled
Nurses are encouraged to voluntarily
accept Dementia Excellence Program
leadership roles and undertake further
study to enhance their clinical expertise.
Staff education also includes topics such
as psychotropic medication use and pain
management. ADementia Excellence
ProgramManager and facilitator provide
expertise and support to site-based
teams. Dementia Excellence focus group
meetings are also held regularly at each
site and include staff, volunteers,
residents and families who work
together to drive change, solve problems
and create action plans.
Lifestyle programs and
tailored support for residents
Every facility has a person-centred
lifestyle program designed to encourage
participation and strengthen
relationships. Things are done ‘with’
residents and not ‘for’ them. Lifestyle
teammembers record residents’ life
stories to better understand each
individual. The Lifestyle Coordinator and
Dementia Excellence Program team, along
with the residents’ Clinical Leaders, also
work together using the Pool Activity
Level (PAL) assessment tool (Pool 2012) to
determine an individual’s level of ability
with activities. Results are used to create a
tailored activity program for each resident
that promotes maximum engagement.
Ongoing family assistance
Eldercare is committed to educating
families. Program information sessions
are held to explain person-centred care
concepts to family members. They’re also
provided with information to increase
their dementia awareness. Furthermore,
site-based chaplains offer care to families
who may be experiencing challenges as
they support loved ones living with
dementia.
Supportive physical environments
Eldercare embraces homely living rather
than the clinical sparseness often
associated with aged care. Our Memory
Support Units (MSUs) have stimulating
items for residents to interact and
connect with. Factors including signage,
lighting and noise as well as room layout
and functionality are regularly reviewed
so the physical environment supports
residents’ cognitive capabilities.
Small changes delivering
dramatic improvements
The Dementia Excellence Program was
introduced three years ago with
Eldercare Evanston Park in Gawler
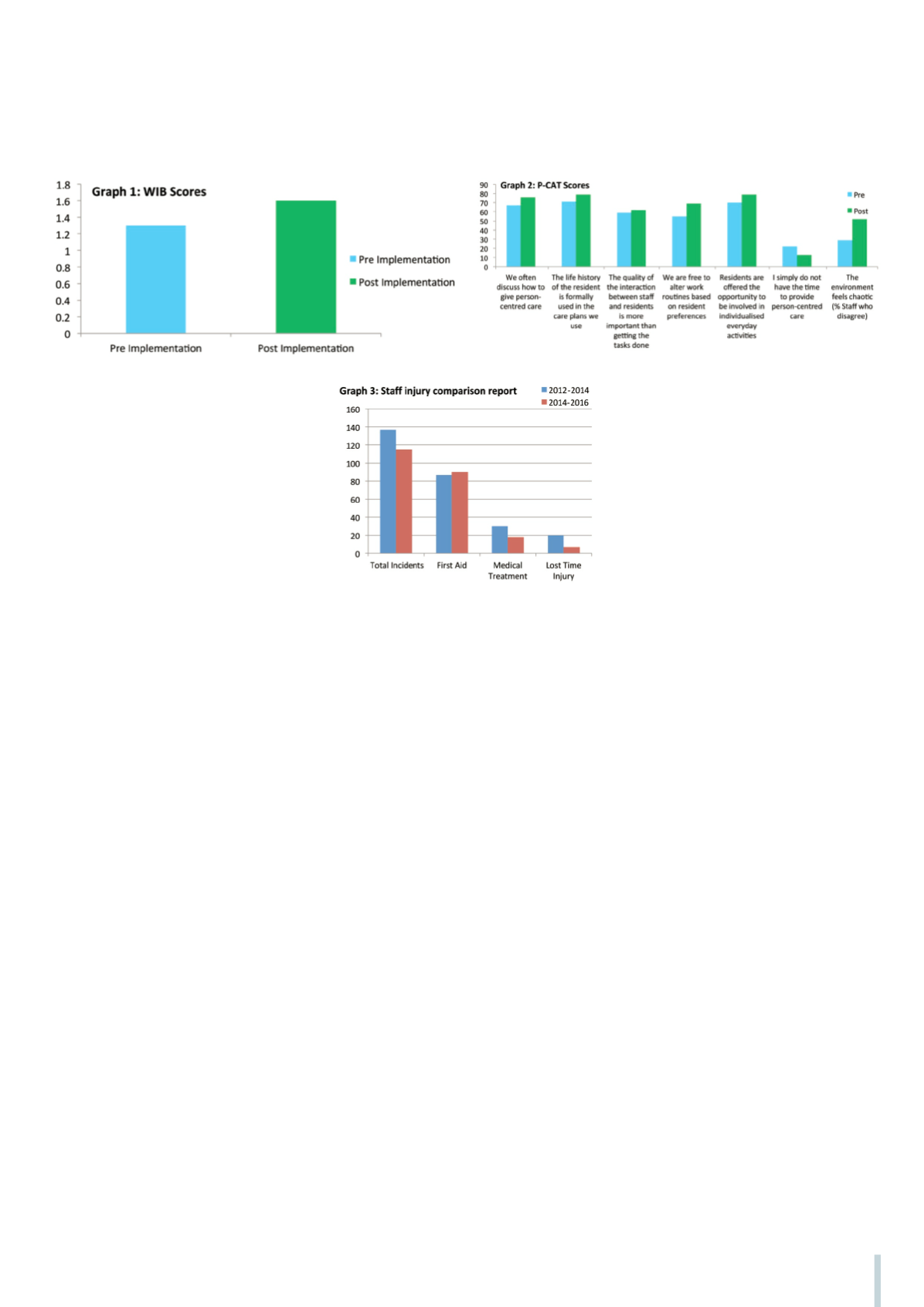
selected as the pilot site. Effectiveness
was evaluated using Dementia Care
Mapping Well and Ill-Being (WIB)
scores (University of Bradford School of
Dementia Studies 2016) for residents
and the Person-Centred Care
Assessment Tool (P-CAT) (La Trobe
University 2013) for staff, with data
collected pre- and post-implementation.
WIB results at Evanston Park showed
residents’ well-being and quality of life
had risen greatly with group scores
increasing from 1.3 at the pre-
implementation stage to 1.7 in post
implementation review. Furthermore,
staff survey outcomes at the trial site
indicated a 20 per cent improvement in
staff attitudes from 65% to 85% with
employees feeling that the care provided
was more genuinely person-centred.
The pilot’s success saw the program
introduced across a further 11 Eldercare
residential aged care facilities between
September 2014 and June 2016. The
encouraging results achieved at
Evanston Park have been reflected across
other sites with additional data proving
that the program is making a positive
difference to resident well-being.
Residents living with dementia in our
MSUs were observed, using the
Dementia Care Mapping (DCM) tool
(University of Bradford 2016), before the
program was implemented and this
process was repeated six months later.
DCM is a process and a tool that is used
to improve the well-being of individuals
living with dementia by observing their
activities, engagement and mood at five
minute intervals across several hours
whilst concurrently watching and
assessing the quality of staff interactions.
The findings are used to support the
development of person-centred care and
create individual strategies to enhance
resident well-being (University of
Bradford 2015).
At three facilities, we were able to map
at further six-monthly intervals
following roll-out at site. In total, 218
residents were mapped before the
program was introduced and 218 were
mapped post implementation across our
MSUs. Some residents were mapped just
the once whilst others were mapped two
or three times.
Of the sites that were mapped pre- and
of person-centred dementia care